STANDARDISED COMPUTED TOMOGRAPHY RADIOMICS COMBINED WITH CLINICAL AND MOLECULAR BIOMARKERS FOR MACHINE LEARNING SURVIVAL PREDICTION IN GLIOMA
ECR2026, Vienna, Avusturya, 4 - 08 Mart 2026, ss.1-6, (Tam Metin Bildiri)
- Yayın Türü: Bildiri / Tam Metin Bildiri
- Basıldığı Şehir: Vienna
- Basıldığı Ülke: Avusturya
- Sayfa Sayıları: ss.1-6
- Dokuz Eylül Üniversitesi Adresli: Evet
Özet
MAIN INFORMATION
Abstract submitted
Abstract accepted
Abstract title
Standardised Computed Tomography Radiomics Combined with Clinical and Molecular Biomarkers for Machine-Learning Survival Prediction in GliomaPreferred Presentation Format
Late-Breaking Poster PresentationPoster Presentation Format
EPOS for Radiologists scientificStudent Presentation Format
-Topic
Artificial IntelligenceFinal Presentation Format
Poster: EPOS Radiologist (scientific)Authors
Z. A. A. Emam1, E. Ada1, O. Cetinayak2, H. C. Koç2, B. Pehlivanoğlu2, K. Akgüngör2, A. Selver1; 1Izmir/TR, 2İzmir/TR
Body
Purpose or Learning Objective
Accurate survival prediction in patients with glioma remains challenging owing to biological and radiological heterogeneity and the complex interplay between imaging appearance, molecular alterations and clinical behaviour; this study evaluated CT-derived radiomic features combined with clinical and molecular biomarkers to develop machine-learning survival models for personalised prognostication.
Methods or Background
A retrospective cohort of 197 glioma patients (subcohort: 154 glioblastoma) who underwent non-contrast CT and had available clinical and molecular data was studied. Tumours were segmented and images underwent standardised preprocessing. From volumes, 107 radiomic features were extracted. Feature-selection pipelines (filter, wrapper and embedded) reduced dimensionality to sets of 5–20 variables. Models evaluated included Cox proportional hazards, elastic-net Cox, random survival forests, gradient-boosting survival and Extra Survival Trees. Models were optimised on development data and tested on an independent set; Harrell’s C-index was the principal metric. In the glioblastoma subgroup we additionally assessed discrimination, calibration, time-dependent AUC and 24-month classification.
Results or Findings
An Extra Survival Trees model with 15 features achieved the highest test C-index (0.731), closely followed by an elastic-net Cox with ten features (0.730). Original NGTDM Coarseness consistently emerged as a dominant radiomic predictor alongside glioblastoma histology, age and IDH status. Feature sets of 10–15 variables offered the best balance between discrimination and generalisability. Mutual-information selection in the glioblastoma cohort yielded C-index 0.65. A Cox model demonstrated independent test discrimination (C-index 0.64; 95% CI 0.52–0.75), significant risk stratification (p < 0.05) and 71.8% accuracy for 24-month survival classification.
Conclusion
Standardised CT radiomic features integrated with clinical and molecular data, using appropriately regularised machine-learning approaches, produce interpretable and clinically meaningful survival predictions to inform personalised management.
Limitations
Limited censored observations and absence of external validation may constrain long-term prediction and generalisability.
Funding for this study
No funding was received for this study.
Has your study been approved by an ethics committee?
YesEthics committee - additional information
The study was approved by Medical Research Ethics Committee of Dokuz Eylul University Hospital (reference number:
2021/22-35, July 28, 2021).
2021/22-35, July 28, 2021).
Multicategories
Hot topic of the year
-Area of Interest
Artificial Intelligence, Head and neck, OncologyImaging Technique
CTProcedure
Diagnostic procedure, Radiation therapy / OncologySpecial Focus
Tissue characterisationReported Cases
Cases Included in Study
Not applicable/If your study includes more than 10 casesSpecify the number of cases
Gallery
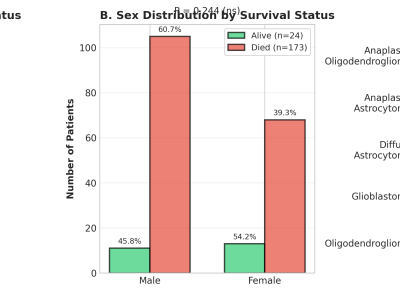
Fig 1: Figure 1. A-C Demographic analysis of patients across surviv...
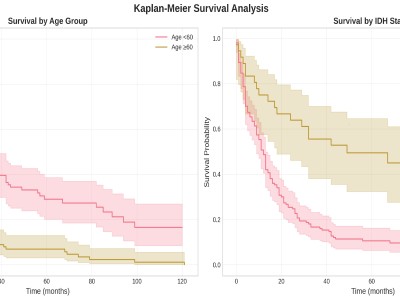
Fig 2: Kaplan–Meier Survival Curves Stratified by Clinical (Age) an...
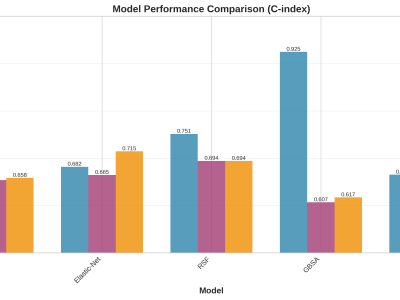
Fig 3: Presents comparative C-index values (training, validation, a...
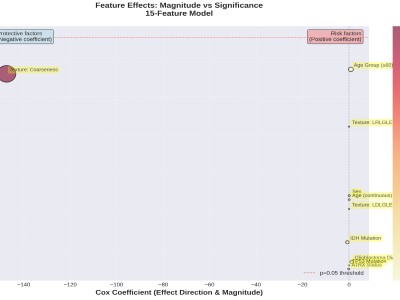
Fig 4: Relationship Between Effect Magnitude and Statistical Signif...
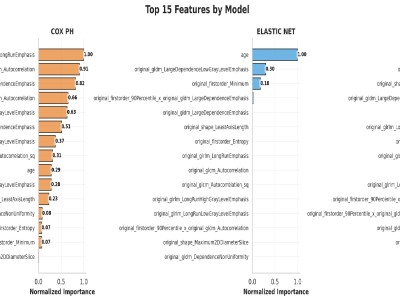
Fig 5: Glioblastoma top 15 mutual predictors by model
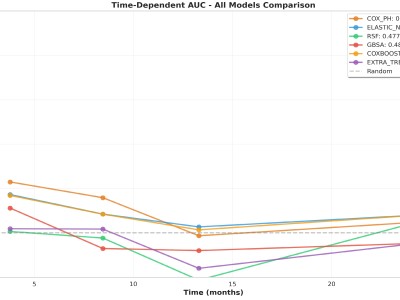
Fig 6: Glioblastoma models evaluation AUC
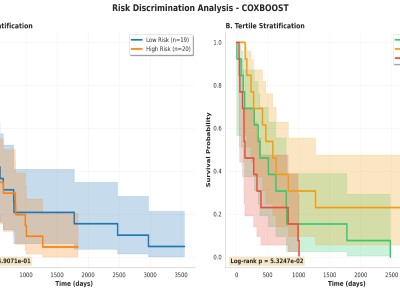
Fig 7: Glioblastoma Cox model Performance on Risk stratification gr...
Usage of AI tools
AI tools used for writing and content editing of the abstract (i.e., editing, grammar, readability, word limit adherence etc.) should be disclosed by checking the AI tool usage box.
This data is collected to reassure reviewers that your AI usage is ethical and transparent. Reviewers will be able to view your indication.
This data is collected to reassure reviewers that your AI usage is ethical and transparent. Reviewers will be able to view your indication.
Affirmations
Material used (mandatory)
I affirm to the ESR that my abstract does not contain any material that is libellous, defamatory, or otherwise unlawful, and that it does not contain any material that invades the right of privacy, any proprietary or copyrights owned.
Patient privacy (mandatory)
I affirm that my abstract does not contain material that reveals patient identity. If there is any chance that a patient can be identified, I confirm to have obtained written informed patient consent for use in this abstract.
Copyright and licenses (mandatory)
I affirm that I have the right to assign license to my work.
I further affirm that if my work contains any material that has been previously published or that is owned by a third party, I was entitled to use this material by applicable law or have obtained a transferable license from the copyright holder.
In case that my study is under evaluation/accepted/published in a scientific journal, I understand that I am advised to consult the respective editorial office regarding copyright and license issues. I also affirm that I will acknowledge in writing (i.e. on a slide or poster, not limited to verbal acknowledgement) the interim (i.e. between abstract submission and congress presentation) acceptance/publication of the study in a scientific journal during my presentation at ECR 2026.
Co-authors agreement (mandatory)
If my abstract is submitted on behalf of co-authors, I warrant that I was given authorisation to represent the other co-authors (co-licensors) as listed in the author line of this abstract.
Presenter registration (mandatory)
I understand that the presenting author of each accepted abstract has to register for ECR 2026 in order to hold a presentation at the congress or have a poster presentation during congress and/or permanently published.
Abstract & Poster publication (mandatory)
I understand that if this abstract is accepted as oral presentation, it will be published in the ECR 2026 Book of Abstracts (as a supplement to "Insights into Imaging", open access under the Creative Commons Attribution License 4.0).
I understand that if this abstract is accepted as a poster, I will have to upload the digital material of my poster to EPOS™ within the given deadline. I acknowledge that the option to permanently publish my poster will be available after the congress, which will include registration with a DOI (digital object identifier) and publication under an open license as outlined in the agreement for the use of EPOS.
I understand that all abstracts which are accepted in a session during ECR 2026 will be displayed in the programme on the ECR online platform before/during the congress.
I understand that all poster presentations at ECR 2026 will be displayed on the ECR login-protected online platform during the congress.